![]()
[2024年08月] を試そう!リアルCDIP問題集で100%無料CDIP試験問題集
CDIPのPDF問題集試験問題 有効なCDIP問題集
質問 # 70
Which of the following demonstrates the relative severity and complexity of patient treated in the hospital, and is used to evaluate the financial impact of a hospital's clinical documentation integrity (CDI) program?
- A. Program for evaluating payment patterns electronic report
- B. Adjusted case mix index
- C. Present on admission indicators
- D. Hospital acquired conditions
正解:B
解説:
Explanation
According to the AHIMA CDIP Exam Preparation Guide, the adjusted case mix index (CMI) is a measure that demonstrates the relative severity and complexity of patients treated in a hospital, and is used to evaluate the financial impact of a hospital's clinical documentation integrity (CDI) program1. The adjusted CMI is calculated by multiplying the unadjusted CMI by a factor that accounts for the percentage of Medicare patients in the hospital2. The higher the adjusted CMI, the higher the expected reimbursement per patient, and the more effective the CDI program is assumed to be3. The other options are not correct because they do not measure the severity and complexity of patients or the financial impact of CDI. Hospital acquired conditions (HACs) are conditions that are not present on admission and are considered preventable by CMS, and may result in reduced reimbursement or penalties4. The program for evaluating payment patterns electronic report (PEPPER) is a report that provides hospital-specific data on potential overpayments or underpayments for certain services or diagnoses, and helps identify areas of risk or opportunity for improvement. Present on admission (POA) indicators are codes that indicate whether a condition was present at the time of admission or acquired during the hospital stay, and affect the assignment of DRGs and HACs. References:
CDIP Exam Preparation Guide - AHIMA
Demystifying and communicating case-mix index - ACDIS
What is Case Mix Index? | The Importance of CMI
Hospital-Acquired Conditions (HACs) | CMS
[PEPPER Resources]
[Present on Admission Reporting Guidelines - CMS]
質問 # 71
In order to best demonstrate the impact of clinical documentation on severity of illness and risk of mortality, which of the following examples is the most effective for physicians in a hospital?
- A. Examples from the hospital's actual cases
- B. Emphasize the Medicare requirements for documentation
- C. The latest Medicare Provider and Analysis Review data
- D. Explanations on how severity of illness and risk of mortality impact reimbursement
正解:A
解説:
Explanation
In order to best demonstrate the impact of clinical documentation on severity of illness and risk of mortality, examples from the hospital's actual cases are the most effective for physicians in a hospital. Examples from the hospital's actual cases can show how specific documentation elements, such as diagnoses, procedures, complications, comorbidities, and present on admission indicators, can affect the severity of illness and risk of mortality scores of the patients, as well as the hospital's performance and reputation. Examples from the hospital's actual cases can also provide feedback and education to the physicians on how to improve their documentation practices and standards. References: :
https://www.ahima.org/media/owmhxbv1/cdip_contentoutline_2023_final.pdf :
https://my.ahima.org/store/product?id=67077
質問 # 72
A patient receives a blood transfusion after a 400 ml blood loss during surgery. The clinical documentation integrity practitioner (CDIP) queries the physician for an associated diagnosis. The facility does not maintain queries as part of the permanent health record. What does the physician need to document for the CDIP to record the query as answered and agreed?
- A. The associated diagnosis and the clinical rationale in the progress notes
- B. The associated diagnosis directly on the query form
- C. A cause-and-effect relationship between anemia and the underlying cause
- D. That the blood loss was not clinically significant
正解:A
解説:
Explanation
The physician needs to document the associated diagnosis and the clinical rationale in the progress notes for the CDIP to record the query as answered and agreed because this is the best way to ensure that the health record reflects the patient's condition and treatment accurately and completely. The associated diagnosis is the condition that caused or contributed to the blood loss and the need for transfusion, such as acute blood loss anemia, hemorrhage, or trauma. The clinical rationale is the explanation of how the diagnosis is supported by the clinical indicators, such as laboratory values, vital signs, symptoms, or procedures. Documenting the associated diagnosis and the clinical rationale in the progress notes also helps to avoid any confusion or inconsistency with other parts of the health record, such as the discharge summary or the coding. (CDIP Exam Preparation Guide) References:
CDIP Exam Content Outline1
CDIP Exam Preparation Guide2
Guidelines for Achieving a Compliant Query Practice (2019 Update)3
質問 # 73
A noncompliant query includes querying the provider regarding
- A. morbid obesity due to BMI of 40.9 documented on the history and physical
- B. gram-negative pneumonia on every pneumonia case, regardless of documented clinical indicators
- C. sepsis that was present on admission because sepsis was only documented in the discharge summary
- D. acute blood loss anemia due to low hemoglobin treated with iron supplements
正解:B
解説:
Explanation
A noncompliant query includes querying the provider regarding gram-negative pneumonia on every pneumonia case, regardless of documented clinical indicators because it may lead to over-specification of a diagnosis that is not supported by the health record. A compliant query should be based on the clinical evidence and documentation in the record, and should not suggest or imply a diagnosis that is not clinically relevant or plausible. A query should also not be driven by reimbursement or coding factors, but by the need to improve the quality and accuracy of documentation. (CDIP Exam Preparation Guide) References:
CDIP Exam Content Outline1
CDIP Exam Preparation Guide2
Guidelines for Achieving a Compliant Query Practice (2019 Update)3
質問 # 74
Whether or not queries should be kept as a permanent part of the medical record is decided by
- A. federal law
- B. physician preference
- C. state law
- D. organizational policy
正解:D
解説:
Explanation
According to the AHIMA/ACDIS Query Practice Brief, whether or not queries should be kept as a permanent part of the medical record is decided by the organizational policy of each facility1. There is no federal or state law that mandates the retention of queries in the medical record, although some external reviewers may request copies of queries to validate the query wording and compliance2. Physician preference is not a valid factor in determining the query retention policy, as queries should be handled consistently across the organization3. Therefore, the correct answer is D. organizational policy. References:
Guidelines for Achieving a Compliant Query Practice (2019 Update) - AHIMA Q&A: Develop policies regarding query retention | ACDIS Q&A: Keep query retention policies consistent | ACDIS
質問 # 75
The clinical documentation integrity (CDI) manager is reviewing physician benchmarks and notices a low-severity level being measured against average length of stay.
What should the CDI manager keep in mind when discussing this observation with physicians?
- A. The diagnosis with a higher degree of specificity has a lower severity of illness.
- B. The query rate is too high while the agreement rate is low.
- C. The query response rate directly correlates to quality reports.
- D. The indicator is a key factor of measurement for quality reports.
正解:D
解説:
Explanation
According to the AHIMA CDIP Exam Preparation Guide, one of the CDI metrics and statistics that CDI managers should track and interpret is the severity level measured against average length of stay (ALOS)1. This indicator reflects the complexity and acuity of the patient population and the quality of care provided by the hospital2. A low-severity level with a high ALOS may indicate under-documentation or under-coding of the patient's condition, which may affect the hospital's reimbursement, risk adjustment, and quality scores3. Therefore, the CDI manager should keep in mind that this indicator is a key factor of measurement for quality reports when discussing this observation with physicians, and educate them on the importance of documenting and coding accurately and completely to reflect the patient's true severity of illness. The other options are not correct because they do not address the issue of severity level measured against ALOS, or they are not relevant to the CDI manager's role or responsibility. References:
CDIP Exam Preparation Guide - AHIMA
Demystifying and communicating case-mix index - ACDIS
Severity of Illness: What Is It? Why Is It Important? | HCPro
質問 # 76
The BEST place for the provider to document a query response is which of the following?
- A. The query form
- B. An addendum to the history and physical
- C. The next progress note and all subsequent notes including the discharge summary
- D. The next progress note and the problem list
正解:D
解説:
Explanation
The best place for the provider to document a query response is the next progress note and the problem list because this ensures that the query response is timely, consistent, and integrated into the health record. According to the AHIMA/ACDIS query practice brief1, the provider should document the query response in the health record as soon as possible after receiving the query, preferably in the next progress note.
The provider should also update the problem list to reflect any new or revised diagnoses resulting from the query response. This helps to maintain an accurate and comprehensive list of the patient's current and chronic conditions, which can facilitate continuity of care, quality reporting, and reimbursement. Documenting the query response in an addendum to the history and physical or only on the query form is not sufficient, as it may not capture the current status of the patient or be easily accessible to other providers or coders.
References:
CDIP Exam Content Outline (https://www.ahima.org/media/1z0x0x1a/cdip-exam-content-outline.pdf) Guidelines for Achieving a Compliant Query Practice-2022 Update1
質問 # 77
Which of the following should be shared to ensure a clear sense of what clinical documentation integrity (CDI) is and the CDI practitioner's role within the organization?
- A. Milestones
- B. Mission
- C. Review schedule
- D. Productivity standards
正解:B
解説:
Explanation
Sharing the mission of the CDI program should be done to ensure a clear sense of what CDI is and the CDI practitioner's role within the organization. The mission statement defines the purpose, goals, and values of the CDI program, and how it aligns with the organization's vision and strategy. The mission statement also communicates the benefits and expectations of the CDI program to various stakeholders, such as providers, executives, coders, quality staff, and patients. The mission statement can help establish the credibility, professionalism, and identity of the CDI practitioners, and guide their daily activities and decisions 2.
References: 1: AHIMA CDIP Exam Prep, Fourth Edition, p. 133 3 2: Mission CDI: Guiding goals, values, and principles 1
質問 # 78
After one year, the clinical documentation integrity (CDI) program has become stagnant, and the manager plans to reinvigorate the program to better reflect the CDI efforts in the organization. What can the manager do to ensure program success?
- A. Expand the CDI program to larger areas in outpatient clinics
- B. Prioritize to focus on efforts with the largest return on investment
- C. Identify key metrics to develop program measures for coders
- D. Establish a CDI steering committee to build a strong foundation
正解:D
解説:
Explanation
A CDI steering committee is a group of interdisciplinary leaders who oversee and guide the CDI program's objectives, outcomes, and metrics. The committee should include representatives from finance, clinical, coding, quality, and other areas that are impacted by CDI. The committee should meet regularly to review the CDI program's performance, identify opportunities for improvement, and provide support and education to the CDI staff and providers. A CDI steering committee can help reinvigorate a stagnant CDI program by ensuring that it aligns with the organization's vision and mission, addresses the current challenges and needs, and fosters collaboration and communication among stakeholders. The other options are not necessarily effective ways to reinvigorate a CDI program. Expanding the CDI program to larger areas in outpatient clinics may not be feasible or appropriate without a clear strategy and plan. Prioritizing to focus on efforts with the largest return on investment may not reflect the true value and quality of the CDI program. Identifying key metrics to develop program measures for coders may not capture the full scope and impact of the CDI program.
質問 # 79
What is the term used when a patient is entered in the Master Patient Index (MPI) multiple times, in different ways, resulting in multiple medical record numbers?
- A. Clone
- B. Facsimile
- C. Overlap
- D. Replica
正解:C
解説:
Explanation
The term used when a patient is entered in the MPI multiple times, in different ways, resulting in multiple medical record numbers is overlap. An overlap occurs when a person has more than one medical record number within an integrated delivery network or enterprise, and may cause problems such as incomplete or inaccurate patient information, duplicate testing or treatment, billing errors, or patient safety issues. An overlap may be caused by data entry errors, system conversions, mergers or acquisitions, or lack of standardization. Regular audits of the MPI database must be done to identify and resolve any overlaps and ensure data quality and integrity.
References:
CDIP Exam Content Outline (https://www.ahima.org/media/1z0x0x1a/cdip-exam-content-outline.pdf) Master patient index - Clinfowiki1
質問 # 80
A patient presents to the emergency room with acute shortness of breath. The patient has a history of lung cancer that has been treated previously with radiation and chemotherapy. The patient is intubated and placed on mechanical ventilation. A chest x-ray is remarkable for a pleural effusion. A thoracentesis is performed, and the cytology results show malignant cells. Diagnoses on discharge: Acute respiratory failure due to recurrence of small cell carcinoma and malignant pleural effusion. Which coding reference takes precedence for assigning the ICD-10-CM/PCS codes?
- A. ICD-10-CM Official Guidelines for Coding and Reporting
- B. Conventions and instructions of the classification for ICD-10-CM/PCS
- C. AHA Coding Clinic for ICD-10-CM/PCS
- D. AMA CPT Assistant
正解:B
解説:
Explanation
According to the CDIP Exam Content Outline, one of the tasks of a clinical documentation integrity practitioner (CDIP) is to apply coding conventions, guidelines, and definitions for ICD-10-CM/PCS. Coding conventions are the general rules for the use of the classification system, such as the use of abbreviations, punctuation, symbols, and sequencing instructions. Coding guidelines are the official rules for selecting and reporting codes based on the documentation in the health record. Coding definitions are the explanations of the terms and concepts used in the classification system. The conventions and instructions of the classification for ICD-10-CM/PCS take precedence over any other coding reference because they are the primary source of coding rules and standards. The other coding references, such as AMA CPT Assistant, AHA Coding Clinic for ICD-10-CM/PCS, and ICD-10-CM Official Guidelines for Coding and Reporting, are secondary sources that provide additional guidance, clarification, or interpretation of the coding conventions and instructions.
References:
CDIP Exam Content Outline (https://www.ahima.org/media/1z0x0x1a/cdip-exam-content-outline.pdf) ICD-10-CM Features | Diagnosis Coding: Using the ICD-10-CM1
質問 # 81
Based on the flowchart below, at what point might the clinical documentation integrity practitioner (CDIP) enlist the help of the physician advisor/champion?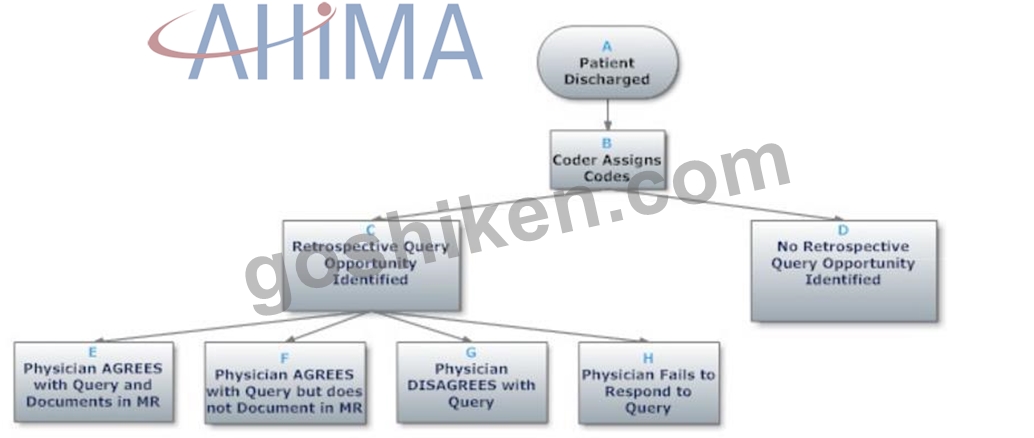
- A. D - No retrospective query opportunity identified
- B. H - Physician fails to respond tocquery
- C. E - Physician agrees with query and documents in MR
- D. C - Retrospective query opportunity identified
正解:B
質問 # 82
A 90-year-old female patient was admitted to emergency room c/o nausea and vomiting x2 days. Vital signs:
BP 130/72, P 86, R 22, T 99.8F, O2 sat 94% on room air. Patient has a history of cerebral vascular accident (CVA) and difficulty swallowing. CXR revealed right lower lobe infiltrate. Labs: WBC 12.0 with 71% segs. Physician documents patient with a history of CVA and difficulty swallowing. CXR revealed right lower lobe infiltrate, diagnosis: pneumonia.
Aspiration precautions and IV Clindamycin
ordered. Patient was discharged 3 days later with a diagnosis of pneumonia. Clarification is needed to determine which of the following is clinically indicated.
- A. Simple pneumonia
- B. Aspiration pneumonia
- C. Pneumonia, a sequela of CVA
- D. Complex pneumonia
正解:B
解説:
Explanation
Aspiration pneumonia is a type of pneumonia that occurs when food, saliva, liquids, or vomit is breathed into the lungs or airways leading to the lungs, causing an infection or inflammation. Aspiration pneumonia is more likely to occur in people who have difficulty swallowing, such as those with a history of CVA2. In this case, the patient has a history of CVA and difficulty swallowing, and presents with nausea and vomiting, which are risk factors for aspiration. The CXR reveals a right lower lobe infiltrate, which is a common finding in aspiration pneumonia3. The physician documents pneumonia as the diagnosis, but does not specify the type or cause. Therefore, clarification is needed to determine if aspiration pneumonia is clinically indicated, as it would affect the coding and reimbursement of the case. Aspiration pneumonia is coded as ICD-10-CM code J69.x Pneumonitis due to solids and liquids, with a fourth digit required to specify the inhaled substance4.
References:
CDI Week 2020 Q&A: CDI and key performance indicators1
Mayo Clinic: Aspiration pneumonia2
Medscape: Aspiration Pneumonia3
ICD-10-CM Diagnosis Code J69.x: Pneumonitis due to solids and liquids4
質問 # 83
A patient is admitted for chronic obstructive pulmonary disease (COPD) exacerbation. The patient is on 3L of home oxygen and is treated during admission with 3L of oxygen. The most appropriate action is to
- A. query the provider to see if chronic respiratory failure is supported by the health record
- B. query the provider to see if acute on chronic respiratory failure is supported by the health record
- C. code the diagnoses of COPD exacerbation and chronic respiratory failure
- D. query the provider to see if respiratory insufficiency is supported by the health record
正解:B
解説:
Explanation
According to the AHIMA/ACDIS Query Practice Brief, one of the scenarios that warrants a query is when there is clinical evidence of a higher degree of specificity or severity1. In this case, the patient's COPD exacerbation and oxygen therapy may indicate a higher level of respiratory impairment than chronic respiratory failure alone. Therefore, a query to the provider to see if acute on chronic respiratory failure is supported by the health record is appropriate and compliant. Acute on chronic respiratory failure is a more specific and severe diagnosis that may affect the patient's severity of illness, risk of mortality, and reimbursement2. The other options are not correct because they either assume a diagnosis without querying the provider, or query for a less specific or severe diagnosis than what the clinical indicators suggest.
References:
Guidelines for Achieving a Compliant Query Practice (2019 Update) - AHIMA Q&A: Respiratory failure in a drug overdose | ACDIS
質問 # 84
Which of the following criteria for clinical documentation means the content of the record is trustworthy, safe, and yielding the same result when repeated?
- A. Reliable
- B. Legible
- C. Complete
- D. Precise
正解:A
解説:
Explanation
According to AHIMA, clinical documentation is at the core of every patient encounter and it must be meaningful to accurately reflect the patient's disease burden and scope of services provided. In order to be meaningful, the documentation must be clear, consistent, complete, precise, reliable, timely, and legible1. Reliability is one of the criteria for clinical documentation that means the content of the record is trustworthy, safe, and yielding the same result when repeated1. Reliability ensures that the documentation is consistent with the clinical evidence and reasoning, and that it can be verified by other sources or methods. Reliability also implies that the documentation is free from errors, omissions, contradictions, or ambiguities that could compromise its validity or usefulness1.
References:
Clinical Documentation Integrity Education & Training | AHIMA1
質問 # 85
A 56-year-old male patient complains of feeling fatigued, has nausea & vomiting, swelling in both legs.
Patient has history of chronic kidney disease (CKD) stage III,
coronary artery disease (CAD) & hypertension (HTN). He is on Lisinopril. Vital signs: BP 160/80, P 84, R 20, T 100.OF. Labs: WBC 11.5 with 76% segs, GFR 45. CXR showed slight left lower lobe haziness. Patient was admitted for acute kidney injury (AKI) with acute tubular necrosis (ATN). He was scheduled for hemodialysis the next day. Two days after admission patient started coughing, fever of 101.8F, CXR showed left lower lobe infiltrate, possible pneumonia. Attending physician documented that patient has pneumonia and ordered Rocephin IV. How should the clinical documentation integrity practitioner (CDIP) interact with the physician to clarify whether or not the pneumonia is a hospital-acquired condition (HAC)?
- A. No need to query the physician because even if the pneumonia is considered a HAC and cannot be used as an MCC, ATN is also an MCC.
- B. Dr. Adair, please indicate if the patient's pneumonia was present on admission (POA) based on the initial chest x-ray?
- C. No need to interact with the physician because it is obvious the pneumonia developed after admission, therefore, not present on admission.
- D. Dr. Adair, in your clinical opinion, do you think that the patient's acute kidney injury with ATN exacerbated the patient's pneumonia?
正解:B
解説:
Explanation
The clinical documentation integrity practitioner (CDIP) should interact with the physician to clarify whether or not the pneumonia is a hospital-acquired condition (HAC) by asking the physician to indicate if the pneumonia was present on admission (POA) based on the initial chest x-ray. This is because the POA status of a condition affects its coding, reporting, and reimbursement, and it is the responsibility of the physician to document the POA status of all diagnoses. The CDIP should not assume that the pneumonia developed after admission based on the timing of symptoms or treatment, as this may not reflect the true clinical picture. The CDIP should also not ask the physician about the causal relationship between the acute kidney injury and the pneumonia, as this is not relevant to the POA status. The CDIP should also not avoid querying the physician based on the presence of another MCC, as this may compromise the accuracy and completeness of documentation. (CDIP Exam Preparation Guide) References:
CDIP Exam Content Outline
CDIP Exam Preparation Guide
Present on Admission Reporting Guidelines
質問 # 86
When there is a discrepancy between the clinical documentation integrity practitioner's (CDIP's) working DRG and the coder's final DRG, which of the following is considered a fundamental element that must be in place for a successful resolution?
- A. Coder and CDIP interaction
- B. Physician and CDIP interaction
- C. Executive oversight
- D. Physician advisor/champion involvement
正解:A
解説:
Explanation
According to the AHIMA/ACDIS Query Practice Brief, one of the fundamental elements that must be in place for a successful DRG discrepancy resolution is a collaborative and respectful interaction between the coder and the CDIP1. The coder and the CDIP should communicate effectively and timely to identify and resolve any DRG mismatches, using evidence-based guidelines, coding conventions, and query standards1. The coder and the CDIP should also share their knowledge and expertise with each other, and seek clarification from the provider or the physician advisor/champion when necessary1. The other options are not considered fundamental elements for DRG discrepancy resolution, although they may be helpful or supportive in some situations. References:
Guidelines for Achieving a Compliant Query Practice (2019 Update) - AHIMA
質問 # 87
A 77-year-old male with chronic obstructive pulmonary disease (COPD) is admitted as an inpatient with severe shortness of breath. The patient is placed on oxygen at 2 liters per minute via nasal cannula. History reveals that the patient is on oxygen nightly at home. CXR is unremarkable. The most compliant query is
- A. Patient has COPD and is on oxygen every night at home and has been on continuous oxygen since admission. Based on these indications, please document chronic respiratory failure, acute respiratory failure, acute on chronic respiratory failure.
- B. Patient has COPD, and is on nocturnal oxygen at home and is on continuous oxygen since admission.
Please indicate if you are treating one of these diagnoses: chronic respiratory failure, acute respiratory failure, acute on chronic respiratory failure, unable to determine, other. - C. Patient has COPD and is on oxygen every night at home and has been on continuous oxygen since admission, please document chronic respiratory failure, hypoxia, acute on chronic respiratory failure.
- D. Patient has COPD, and is on nocturnal oxygen at home and is on continuous oxygen since admission.
Please order further tests so the patient's severity of illness can be captured with the most accurate coding assignment.
正解:B
解説:
Explanation
According to the AHIMA/ACDIS Query Practice Brief, a compliant query should provide multiple choice answer options that are supported by clinical indicators and include a non-leading query statement1. Option C meets these criteria, as it provides a list of possible diagnoses that are relevant to the patient's condition and asks the provider to indicate which one they are treating. Option C also does not imply or suggest a preferred answer or outcome, and allows the provider to choose unable to determine or other if none of the listed options apply. Option A is not compliant, as it does not provide any answer options and implies that the provider should order more tests to capture a higher severity of illness. Option B is not compliant, as it provides only one answer option and suggests that the provider should document it based on the clinical indicators. Option D is not compliant, as it provides only one answer option and implies that the provider should document it based on the indications. References:
Guidelines for Achieving a Compliant Query Practice (2019 Update) - AHIMA
質問 # 88
An organization dealing with staffing shortages has adopted a policy requiring clinical documentation integrity practitioner (CDIP) to stop reviewing any record after a major complication or co-morbidity is found. What is the unintended consequence of this?
- A. Decrease in severity of illness and risk of mortality
- B. Reduced risk of clinical denials
- C. Increase in case mix index
- D. Increased number of records reviewed by each CDIP
正解:A
解説:
Explanation
Severity of illness (SOI) and risk of mortality (ROM) are two metrics that measure the complexity and acuity of a patient's condition, based on the number, nature, and interaction of complications and comorbidities (CCs) and major CCs (MCCs). SOI reflects the extent of physiologic decompensation or organ system loss of function, while ROM reflects the likelihood of dying. Both SOI and ROM are divided into four levels: minor, moderate, major, or extreme. These metrics are used to adjust payment rates, quality indicators, and performance measures for hospitals and other healthcare providers.
If a CDIP stops reviewing any record after a major CC is found, they may miss other CCs or MCCs that could affect the patient's SOI and ROM levels. For example, a patient with pneumonia and sepsis would have a major CC (pneumonia) and an MCC (sepsis). If the CDIP stops reviewing the record after finding pneumonia, they would not capture sepsis, which would increase the patient's SOI and ROM levels from major to extreme.
This would result in underreporting the patient's true complexity and acuity, and potentially lead to lower reimbursement, lower quality scores, and higher denial risk.
Therefore, the unintended consequence of this policy is a decrease in SOI and ROM levels for patients who have more than one CC or MCC.
References:
CDIP Exam Preparation Guide, 2021 Edition. AHIMA Press. ISBN: 9781584268530 Q&A: Understanding SOI and ROM in the APR-DRG system
3M™ All Patient Refined Diagnosis Related Groups (APR DRGs)
Severity of illness | definition of severity of illness by Medical dictionary Using Severity Adjustment Classification for Hospital Internal and External Comparisons
質問 # 89
A patient falls off a ladder and undergoes a right femur procedure. Three weeks later, the patient returns to the hospital for removal of the external fixation device. The ICD-10-CM 7th character code value should indicate
- A. subsequent
- B. initial
- C. sequela
- D. aftercare
正解:D
解説:
Explanation
The ICD-10-CM 7th character code value should indicate aftercare for a patient who falls off a ladder and undergoes a right femur procedure, and then returns to the hospital for removal of the external fixation device.
Aftercare codes are used to capture encounters for follow-up care after completed treatment of an injury or condition, such as removal of external fixation devices, casts, or pins. Aftercare codes are not used for subsequent encounters for complications or infections related to the injury or condition5 References: 1:
https://www.ahima.org/media/owmhxbv1/cdip_contentoutline_2023_final.pdf 5:
https://my.ahima.org/store/product?id=67077
質問 # 90
Which of the following sources provide external benchmarks to examine the effectiveness of a facility's clinical documentation program?
- A. Health Care Financing Administration
- B. Agency for Healthcare Research and Quality
- C. Medicare Provider Analysis and Review
- D. American Health Information Management Association
正解:B
解説:
Explanation
The Agency for Healthcare Research and Quality (AHRQ) provides external benchmarks to examine the effectiveness of a facility's clinical documentation program by developing and disseminating quality indicators (QIs) that measure various aspects of health care quality, such as patient safety, outcomes, efficiency, and effectiveness. These QIs are based on administrative data and can be used to compare the performance of different health care providers or facilities across the nation. The QIs include inpatient quality indicators (IQIs), patient safety indicators (PSIs), prevention quality indicators (PQIs), and pediatric quality indicators (PQIs). These QIs can help clinical documentation improvement (CDI) programs identify areas of improvement, monitor trends, and evaluate the impact of CDI interventions on health care quality 2.
References: 1: Clinical Documentation Improvement Programs: Quality, Efficiency | Deloitte US Analysis 2 2:
AHRQ Quality Indicators 3
質問 # 91
The physician advisor/champion needs to provide ongoing education regarding coding and reimbursement regulations to the
- A. clinical documentation integrity staff
- B. Health Information Management coding staff
- C. organization's medical and surgical staff
- D. organization senior administration staff
正解:C
解説:
Explanation
The physician advisor/champion is a key role in the CDI program who serves as a liaison between the CDI staff and the organization's medical and surgical staff. The physician advisor/champion needs to provide ongoing education regarding coding and reimbursement regulations to the organization's medical and surgical staff to promote awareness, understanding, and compliance with CDI initiatives and goals.
References: AHIMA. "CDIP Exam Preparation." AHIMA Press, Chicago, IL, 2017: 97-98.
質問 # 92
When benchmarking with outside organizations, the clinical documentation integrity practitioner (CDIP) must determine if the organization is benchmarking with which of the following criteria?
- A. Hospitals that are its peers
- B. Hospital within its region
- C. Hospital within its state
- D. Hospital within its county
正解:A
解説:
Explanation
When benchmarking with outside organizations, the clinical documentation integrity practitioner (CDIP) must determine if the organization is benchmarking with hospitals that are its peers because peer hospitals have similar characteristics such as size, location, teaching status, case mix index, and payer mix. Benchmarking with peer hospitals allows for a more accurate and meaningful comparison of performance indicators and outcomes. (CDIP Exam Preparation Guide) References:
CDIP Exam Content Outline1
CDIP Exam Preparation Guide2
質問 # 93
Yes/No queries may be used
- A. to resolve conflicting documentation from multiple practitioners
- B. when only the clinical indicators of a condition are present
- C. when the diagnosis is not clearly documented in the health record
- D. in any query format
正解:A
質問 # 94
......
究極のCDIP無料準備ガイド最新のAHIMA練習テスト問題集:https://www.goshiken.com/AHIMA/CDIP-mondaishu.html
今すぐゲットせよ!高評価AHIMA CDIP試験問題集:https://drive.google.com/open?id=1j-mQFtixy9PsDEILYefsMkMkFv-eMfI_